Held as a side event CUMO annual Congress, the 4P-CAN project convened a policy round table that brought together partners from South-Eastern Europe and the Balkans to address what participants described as the persistent “iron curtain” of prevention inequalities across Europe.
Experts from South-Eastern Europe and the Balkans discussed the growing inequalities in cancer prevention access, health literacy, and policy implementation across the region.
The discussion drew on experiences from Romania, Bulgaria, Moldova, Montenegro, and North Macedonia. Moderated by Mădălina Iamandei of All.Can International, the session also included local Montenegrin stakeholders with expertise spanning medicine, academia, epidemiology, social work, public health authorities, statistics, NGOs, the private sector, the Clinical Centre of Montenegro, and the National Public Health Institute of Montenegro.
The realities from Romania were presented by Marius Geanta, Coordinator of 4P-CAN and President of the Centre for Innovation in Medicine (INOMED), who reflected on Romania’s ongoing struggles with prevention access, implementation, and health literacy. He noted that prevention services are often unavailable outside major cities, that top‑down fragmented policies ignore local realities, and that low health literacy—compounded by poor digital literacy—widens the gap between those who can navigate prevention and those who cannot.
The prevention landscape and inequalities affecting Montenegro were outlined by Dr. Nikola Milasevic from CUMO, who introduced the National Programme for the Prevention and Control of Malignant Diseases with an Action Plan for 2026–2028. This programme aligns with EU accession commitments in health and social policy, follows government methodology, and is grounded in a newly adopted healthcare law that emphasises prevention, digitalisation, and patient‑centred care, building on existing national strategies and international frameworks.
Bulgaria’s unequal cancer prevention landscape was summarised by Ivaylo Petrov, PharmD from the Bulgarian Joint Cancer Network (BJCN), who described fragmented policies, low screening uptake, limited stakeholder coordination, and insufficient use of
data. He highlighted strategic shifts led by the Ministry of Health toward an organised, evidence‑based cancer screening model, a school‑based health promotion framework, and a national cancer registry aligned with European standards.
Key priorities include clear governance, pilot implementation, stronger health literacy and tobacco control, mandatory data submission, and coordinated action among government, healthcare, education, civil society, and European partners.
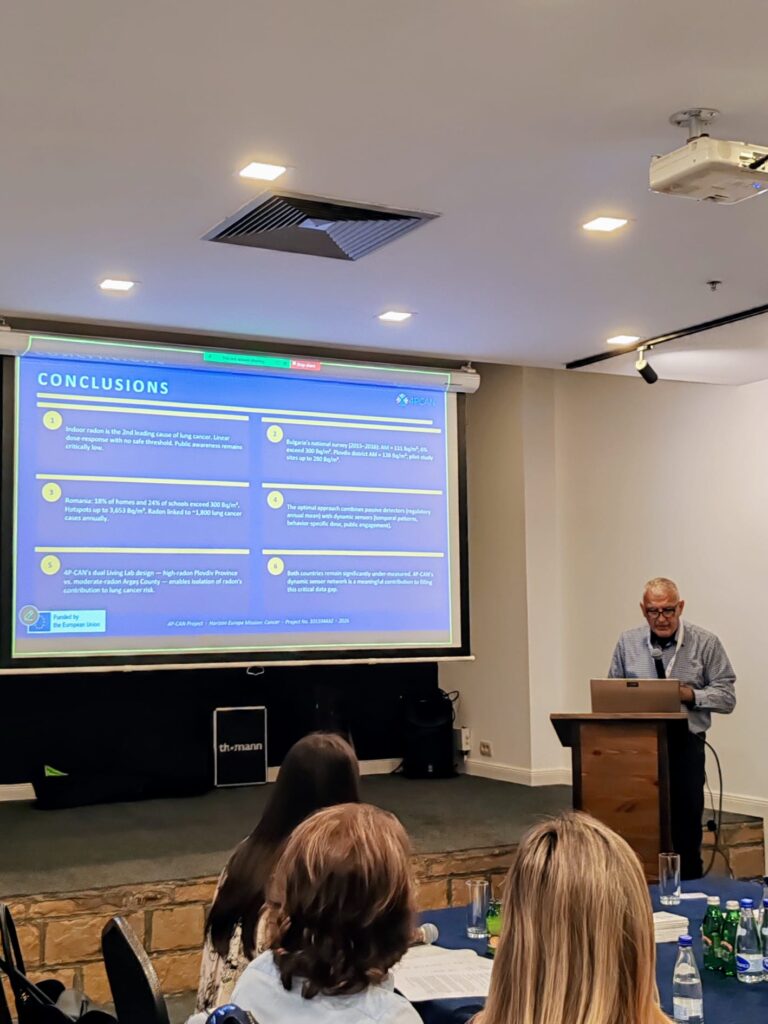
The environmental determinants of health, specifically radon exposure as a major cause of lung cancer, were addressed by Prof. Ivan Tchalakov from the University of Plovdiv Paisii Hilendarski. He provided a comprehensive overview of indoor radon in Bulgaria and Romania, stressing the need for greater public awareness, expanded monitoring, and the role of the 4P‑CAN project in filling critical data gaps.
The patient and community perspective on prevention inequalities and access in North Macedonia was brought forward by Milica Kuzmanovska from the Association for Help and Support of Patients with Gynaecological Diseases FEMINA M, who argued that the
country must shift from fragmented, opportunistic cancer prevention to an integrated, population‑based system within two to three years. This would require a centralised digital registry, systematic invitations, and primary care integration.
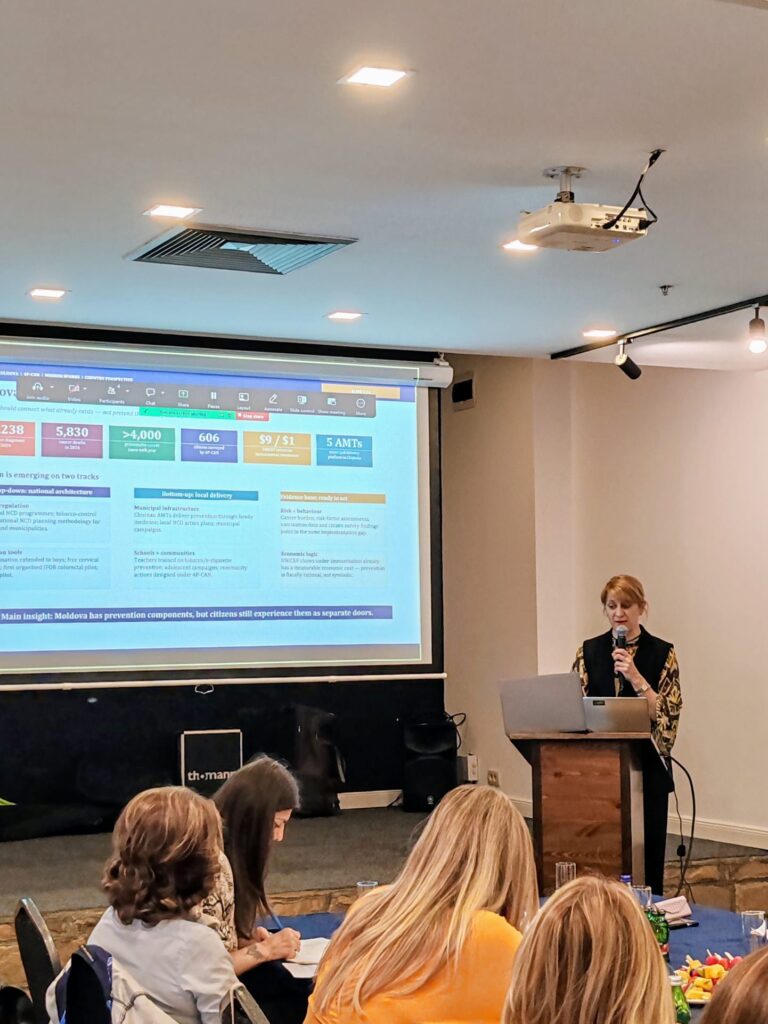
Moldova’s current cancer prevention landscape and proposed strategic shift for
2026–2028 were presented by representatives from the Republic of Moldova involved in local 4P‑CAN activities. They described that while some components exist—such as HPV vaccination, screening pilots, and local delivery through family medicine and municipalities—these remain disconnected, leaving citizens to navigate
the system alone. Evidence from surveys and economic data reveals a gap in active
outreach: prevention exists but is not delivered as a routine, citizen‑centred pathway.
Their goal is to move from a passive model (“services exist”) to an active, list‑based system where the system identifies, invites, delivers, recalls, and corrects prevention efforts, bringing primary prevention to the citizen before they become a patient.
The session highlighted an emerging divide in Europe: inequalities are increasingly rooted in prevention, not only treatment.
Across the region, a common pattern became clear: despite varying health systems, many countries share comparable obstacles, such as disparities in accessing prevention, low levels of health literacy, deficiencies in policy implementation, geographic inequalities, environmental risk factors, and weak community participation in public health efforts.
One key takeaway from the discussion was that cancer inequalities across Europe are no longer defined solely by differences in treatment access—instead, they increasingly stem from uneven access to prevention, reliable information, participation, and effective
implementation.